


HPV – ANOTHER GREAT CAUSE OF ORAL CANCER
-
Shainda Laeeq*1, Dr. Suman Rao Vihari2, Istafa Husain Khan3
*1Lecturer, Department of Pharmacology, Maharana Pratap Dental College, Mandhana, Kanpur.
2Lecturer, Department of Biochemistry, Maharana Pratap Dental College, Mandhana.3Demonstrator, Department of Microbiology, Maharana Pratap Dental College, Mandhana. Email id: shaindalaeeq786@gmail.com
ABSTRACT
HPV oral and oropharyngeal cancers are harder to discover than tobacco related cancers. HPV manifests itself primarily in the posterior regions such as the base of the tongue, the back of the throat, the tonsils, the tonsillar crypts, and tonsillar pillars. HPV is the most common sexually transmitted virus and infection. HPV is driving the growth in numbers of oral cancers every year by about 10%. It can be caused because of the greater number of sexual partners, when engaging in oral sex, this also holds true for oral infections. HPV is passed on through genital contact, most often during vaginal, anal and oral sex. We are more likely to get HPV if we have weakened immune systems also. Many people don't have symptoms and are unaware that they have HPV. The virus may be inactive for weeks, months and for some people possibly even years after infection. The CDC now recommends an HPV test for women along with the PAP test as a matter of routine. Oral HPV testing in both men and women is problematic. There are anal brush cytology tests for those that engage in anal sexual practices.
Keywords: OSCC, dysplasia, human papilloma virus, retinoblastoma, oncogenic -
INTRODUCTION
Over the past 15 years, Human Papilloma Virus (HPV), the necessary cause of cancer of the cervix (Haraf DJ et al., 1996, Paz IB et al., 1997), has also been etiologically linked with a subset of OSCCs (Parkin D M et al 1996., Schwartz SM et al., 1998, Andl T et al.,1998, Gillison ML et al., 2000, Mellin H et al., 2000). Numerous studies provide evidence for casual association between Human Papilloma Virus and a subset of head and neck cancer, similar to cases in anogenital region. (Judit A Nemes 2006). However, in the Western World, HNSCCs, notably of the oral cavity and oropharynx, are becoming more prevalent, which may be related to an increase in oral and oropharyngeal HPV infections (Leeman et al., 2011)
- EPIDEMIOLOGY
The epidemiological studies report a strong association with Human Papilloma Virus (HPV) in a subset of HNSCC. (Head & Neck Squamous Cell cancinoma) More than 95% of cervical squamous cell carcinomas are linked to persistent HPV infection; evidence demonstrates that HPV is a necessary carcinogen. In 2000, head and neck cancer was ranked as the eighth leading cause of cancer death worldwide. Approximately 481,100 new cases developed, and 320,000 persons died of this disease, resulting in an average mortality rate of 7.3 and 3.2 per 100,000 males and females, respectively, The highest worldwide incidence of this disease for females was reported in Bangalore, India, with an average rate of 11.2 cases per 100,000. The worldwide five-year relative survival rate from oral cancer is generally less than 50%, although females tend to have a higher relative survival rate than males. This poor five-year survival rate has remained unchanged for more than three decades (C.C.R. Ragin et al., 2007).
Oral squamous cell carcinomas (OSCC) have broadly varying rates of incidence and mortality around the world, with high rates notably in Southeast Asia and Eastern Europe (Parkin D M et al., 1990). The most common clinically presented malignant lesion of buccal mucosa is oral leukoplakia with a prevalence of 0.1 -0.5 % and rate of transformation to cancer is 1-2 % per year. The treatment and assessment of the risk and progression of leukoplakia remains a problem, as it occurs despite of removal via surgery, and chemotherapy does not decrease cancer incidence (Mondal et al., 2013).
-
RISK FACTORS
It is generally agreed that tobacco, betel quid, alcohol consumption are the major environmental risk factors for developing OSCC. However some patients develop OSCC without exposure to these three risk factors. This fact suggests that the additional causes, such as genetic predisposition, diet or oncogenic viruses, may also help cells to override or escape the physiological mechanism of proliferation control (Judit A Nemes 2006, Brandsma JL et al., 1989).
-
OCCURRENCE, SIGNS AND SYMPTOMS
Oral squamous cell carcinoma amounts for over 90% of all lip and oral cavity malignancies (primarily in the posterior regions such as the base of the tongue, the back of the throat, the tonsils, the tonsillar crypts, and tonsillar pillars).
Symptoms include an ulcer or sore that does not heal within 2-3 weeks, difficult or painful swallowing, painwhen chewing, a persistent sore throat or hoarse voice, a swelling or lump in the mouth, a numb feeling in the mouth or lips, constant coughing, an ear aches on one side unilateral) which persists for more than a few days (Judit A Nemes 2006). A hard/firm, enlarged, painless, fixated node in the neck that has been present for over 21 days should be sampled by fine needle aspiration biopsy at minimum. Lack of symmetry and swelling on one side, which is simultaneously painless when palpated, is a cause for concern, and is not associated with other disease states. This is frequently associated with a positive finding in the cervical nodes on the same side (http://www.oralcancerfoundation.org). -
TYPE OF HPV INVOLVED IN THE ORAL CANCER
As detection of HPV DNA in tumor biopsies alone is not sufficient evidence of causation, molecular biology studies have helped identify a subset of these cancers that may be the consequence of HPV infection (Schwartz SM et al., 1998 , Andl T et al., 1998 , Mork J et al., 2001, Klussmann JP et al., 2001, Ritchie JM et al., 2003 , Snijders PJ et al., 1996 ). Such a subset is mainly found in the oropharynx, particularly the tonsils. Of the 140 HPV types known to infect the mucosal surfaces of the genital tract, 14 are detected in nearly all biopsies of invasive cervical cancer and are therefore considered to be either ''high-risk'' or ''oncogenic'' (Paz IB et al 1997). Some of these high-risk types have also been found in the oral cavity and oropharynx of cancer-free adults (Munger K et al.,1989) and in cancer biopsy specimens from HNSCC patients (Schwartz SM et al.,1998, Andl T et al.,1998, Gillison ML et al., 2000, Mellin H et al., 2000). HPV16, the most prevalent HPV type in cervical SCCs (14), is also the most common type present in HPV-positive HNSCCs (Schwartz SM et al., 1998, Andl T et al.,1998, Gillison ML et al., 2000, Mellin H et al., 2000). -
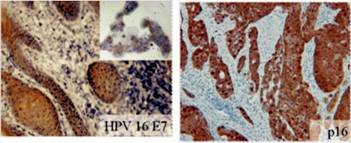
Figure 1– Immunohistochemistry for HPV16 E7 (upper panel) and p16 (lower panel) in representative tumors. HPV16 E7 and p16 staining was detected in the nucleus and the cytoplasm. For HPV16 E7 staining, CasKi cells served as a positive control (upper right corner in the upper panel).Recent studies have suggested an association of SCC to viral pathogens such as high risk (oncogenic) human papilloma virus (HPV) types, particularly HPV16 or 18. (Ritchie JM et al., 2003) These viruses are frequently found in squamous
carcinoma of the head and neck. HPV16 infections have been observed in approximately one half of squamous cell carcinomas of the oropharynx(SCCO).( Gillison ML et al.2000 , Klussmann JP et al., 2001 , Ritchie JM et al., 2003 , Snijders PJ et al.,1996 ) The HPV16 SCCO have a good prognosis and are not associated with conventional risk factors, suggesting they may represent a separate tumor entity.( Haraf DJ et al.,1996 , Gillison ML et al., 2000, Klussmann JP et al., 2001 , Ritchie JM et al., 2003). The HPV-derived oncoproteins E6 and E7 are mainly responsible for both the onset and maintenance of malignant transformation through inactivation of the p53 and retinoblastoma (Rb) tumor suppressor genes, respectively.( Munger K et al.,1989, von Knebel Doeberitz M et al.,1992) Inhibition of Rb protein (pRb) by the HPV16 E7 oncogene product leads to upregulation of p16 via a loss of negative control of pRb expression. Thus, HPV16 E71 SCCO coexpress p16 in nearly 90% of cases, and p16 has been suggested as a surrogate marker for the HPV status in SCCO (Klussmann JP et al., 2003).MODES OF TRANS MISSION OF VIRUS
The Human Papilloma Viruses (HPVs) represent a heterogeneous group of viruses that infect skin and mucosal epithelial tissues. Currently, over 140 genetically different HPV types have been isolated from humans. Humans are the only known reservoirs, and viruses are spread by direct human-to-human contact. Oral SCCs (OSCC) develop from precancerous epithelial dysplasia; the most important steps of the multi step process of carcinogenesis are the activation of oncogenes and the loss of tumour suppressor genes (Judit A Nemes 2006). HPV infection of the larynx is thought to occur through two mechanisms: transmission during passage through an HPV-infected birth canal and through sexual contact. The observed bimodal age distribution of cases, with peaks at age < five and between 20 and 30 years of age, is thought to reflect these two different modes of transmission. Fifty percent of mothers of affected children report a history of genital HPV infection (Shah et al., 1998). In a recent retrospective cohort study based on data in the Danish National Registries, maternal genital warts during pregnancy conferred a greater than 200-fold risk of respiratory papilloma in the child (Silverberg et al., 2003). By contrast, disease among adults has been associated with sexual behaviors such as high numbers of lifetime sexual partners and a
higher frequency of oral sex (Kashima et al.,1993).
-
HPV is one of the most common sexually transmitted diseases (STD) in the world. (American Social Health Association) Condoms do not offer complete protection against HPV infection. The papilloma virus lives in the cells of the outer skin as well as inside the body, mainly in the vagina, anus and urethra. When condoms do not cover the entire shaft of the penis or the pubic skin, papilloma-laden skin cells can easily pass from a man's pubic area into the vagina, vulva or anus (American Social Health Association). HPV does not appear on the standard tests for STD infection that many men and women now routinely undergo when they meet new partners.
- Where there are no visible skin changes, sub-clinical and latent (hidden/inactive) infections can only be detected microscopically within the skin cells via special tests looking for HPV DNA. While there is no pharmacologic cure for HPV, the infection can induce an antibody mediated immune response, which is thought to clear the virus from the body. However, HPV can also effectively evade the body's immune system, residing dormantly (latent infection) inside certain cells or actively infecting cells resulting in the development of warts and/or dysplasias. (Stressgen Biotechnologies Corp. Data on File, 2000).
- Type of the human papillomavirus (HPV), which is sexually transmitted, represents the most important risk factors for cervical cancer (Zur Hausen, 1991). Recent reports show that 30–50% of young women who have recently had sexual intercourse for the first time are infected with HPV in their cervices (Ho et al., 1998; Franco et al., 1999; Molano et al., 2003).
- At the time of the initial infection, there is sometimes, but not always, an eruption of genital warts in either sex that later disappear. The virus may remain latent for many years, and only a few of the infected individuals go on to develop cervical – or oral – cancers later in life. This in itself is an interesting observation, which implies that other genetic and/or environmental factors are involved. HPV-positive oral cancers are excellent candidates for treatment with one of the therapeutic HPV vaccines that are now in clinical trials for cervical cancer (Maura Gillison 2001).
- PREVENTION AND TREATMENT
- Avoid tobacco, smoking, oral sex, undergo vaccination (Gardasil for females) and people who are early detected should undergo chemotherapy, surgery or radiation therapy.
- CONCLUSION
- Oral Squamous cell carcinoma (OSCC) concerned with HPV 16 infection is a leading cause of death in both tobacco and non-tobacco patients. At the time of the initial infection, there is sometimes, but not always, an eruption of genital warts in either sex that later disappear .The virus may remain latent for many years, and lead to develop oral cancer in the infected individuals later in life, so, clinical trials are being done on the vaccine used as preventive measure in cervical cancer to be an excellent candidate for the prevention of oral cancer caused by HPV.
- REFERENCES
- Kreimer, A.R., Clifford, G.M., Boyle, P., Franceschi S. (2005). Human papillomavirus types in head and neck squamous cell carcinomas worldwide: a systematic review. Cancer Epidemiol Biomarkers Prev, 14(2), 467-75.
- Andl, T., Kahn, T., Pfuhl, A., Nicola, T., Erber, R., Conradt, C., Klein, W., Helbig, M., Dietz, A., Weidauer, H., Bosch, FX. (1998). Etiological involvement of oncogenic human papillomavirus in tonsillar squamous cell carcinomas lacking retinoblastoma cell cycle control. Cancer Res, 58(1), 5-13.
- Brandsma, J.L., & Abramson, A.L. (1989). Association of papillomavirus with cancers of the head and neck. Arch Otolaryngol Head Neck Surg, 115(5), 621-5.
- Ragin,C.C.R., Modugno,F.,& Gollin,S.M. (2007). The Epidemiology and Risk Factors of Head and Neck Cancer: a Focus on Human Papillomavirus.J Dent Res, 86(2), 104-114.
- Franco, E.L., Villa, L.L., Sobrinho, J.P., Prado, J.M., Rousseau, M.C., Desy, M., Rohan, T.E. (1999). Epidemiology of acquisition and clearanceof cervical human papillomavirus infection in women from a high-risk area for cervical cancer. J. Infect. Dis, 180, 1415– 1423.
- Gillison, M.L., Koch, W.M., Capone, R.B., Spafford, M., Westra, W.H., Wu, L., Zahurak, M.L., Daniel, R.W., Viglione, M., Symer, D.E., Shah, K.V., Sidransky, D. (2000) Evidence for a causal association between human papillomavirus and a subset of head and neck cancers. J Natl Cancer Inst, 92, 709–20.
- Haraf, D.J., Nodzenski, E., Brachman, D., Mick, R., Montag, A., Graves, D., Vokes, E.E., Weichselbaum, R.R.(1996). Human papilloma virus and p53 in head and neck cancer: clinical correlates and survival. Clin Cancer Res, 2,755–62.
- Ho, G.Y., Bierman, R., Beardsley, L., Chang, C.J., Burk, R.D. (1998). Natural history of cervicovaginal
papillomavirus infection in young women. N. Engl . J.Med , 338, 423- 428. http://www.oralcancerfoundation.org/hpv/ocf-hpv-opinions.php#sthash.wOjfrAD3.dpuf - Judit, A., & Nemes, D.D.S. (2006). Oral Squamous cell carcinoma in north east hungary etiologic and prognostic factors, Ph.D. thesis, university of Debrecen, medical and health science centre, faculty of dentistry.
- Kashima, H., Mounts, P., Leventhal, B., Hruban, R.H. (1993). Sites of predilection in recurrent respiratory papillomatosis. Ann Otol Rhinol Laryngol,102, 580-583.
- Klussmann, J.P., G€ultekin, E., Weissenborn, S.J., Wieland, U., Dries Vdienes, H.P., Eckel, H.E., Pfister, H.J., Fuchs, P.G.(2003). Expression of p16 protein identifies a distinct entity of tonsillar carcinomas associated with human papillomavirus. Am J Pathol, 162,747–53.
- Klussmann, J.P., Weissenborn, S., Wieland, U., Dries, V., Kolligs, J., Jungehuelsing, M., Eckel, H.E., Dienes, H.P., Pfister, H., Fuchs, P. (2001). Prevalence, distribution and viral load of human papillomavirus 16 DNA in tonsillar carcinomas. Cancer, 92, 2875–84.
- Leemans CR, Braakhuis BJ, Brakenhoff RH.(2011). The molecular biology of head and neck cancer. Nat Rev Cancer, 11(1), 9-22.
- Maura Gillison. (2001). Cervical Cancer Virus Linked to Some Head and Neck Cancer. http://oralcancernews.org/wp/cervical-cancer-virus-linked-to-some-head-and-neck-cancer/
- Mellin, H., Friesland, S., Lewensohn, R., Dalianis, T., Munck-Wikland, E. (2000). Human papillomavirus (HPV) DNA in tonsillar cancer: clinical correlates, risk of relapse, and survival. Int J Cancer, 89, 300–4.
- Molano, M., Van den Brule, A., Plummer, M., Weiderpass, E., Posso, H., Arslan, A., Meijer, C.J., Munoz, N., Franceschi, S., HPV Study Group. (2003). Determinants of clearance of human papillomavirus infections in Colombian women with normal cytology: a population-based 5- year follow-up study. Am. J. Epidemiol, 158, 486–494.
- Mondal, P., Data, S., Maiti, G.P., Baral, A., Jha, G.N.(2013). comprehensive SNP scan of DNA damage response genes reveal multiple susceptibility loci conferring risk to tobacco associated leukoplakia and oral cancer.PLoS ONE, 8(2), e56952.
- Mork, J., Lie, A.K., Glattre, E., Hallmans, G., Jellum, E., Koskela, P., Moller, B., Pukkala, E., Schiller, J.T.,
Youngman, L., Lehtinen, M., Dillner, J. (2001). Human papillomavirus infection as a risk factor for squamous-cell carcinoma of the head and neck. N Engl J Med, 344, 1125–31.
- Munger K, Phelps WC, Bubb V, Howley PM, Schlegel R. The E6 and E7 genes of the human papillomavirus type 16 together are necessary and sufficient for transformation of primary human keratinocytes. J Virol 1989; 63:4417–21.
- Parkin DM, Pisani P, Ferlay J. Estimates of the world-wide incidence of 25 major cancers in 1990. Int J Cancer 1999;80:827–41.
- Paz IB, Cook N, Odom-Maryon T, Xie Y, Wilczynski SP. Human papillomavirus (HPV) in head and neck cancer. An association of HPV 16 with squamous cell carcinoma of Waldeyer's tonsillar ring. Cancer 1997;79:595–604
- Ritchie JM, Smith EM, Summersgill KF, Hoffman HT, Wang D, Klussmann JP, Turek LP, Haugen TH. HPV infection as a prognostic factor in carcinomas of the oral cavity and oropharynx. Int J Cancer 2003;104:336–44.
- Schwartz SM, Daling JR, Doody DR,Wipf GC, Carter JJ, Madeleine MM, Mao EJ, Fitzgibbons ED, Huang S, Beckmann AM, McDougall JK, Galloway DA. Oral cancer risk in relation to sexual history and evidence of human papillomavirus infection. J Natl Cancer Inst 1998; 90:1626–36.
- Shah KV, Stern WF, Shah FK, Bishai D, Kashima HK (1998). Risk factors for juvenile onset recurrent respiratory papillomatosis. Pediatr Infect Dis J 17:372-376.
- Silverberg MJ, Thorsen P, Lindeberg H, Grant LA, Shah KV (2003). Condyloma in pregnancy is strongly predictive of juvenile onset recurrent respiratory papillomatosis. Obstet Gynecol 101:645-652.
- Snijders PJ, Scholes AG, Hart CA, Jones AS, Vaughan ED, Woolgar JA, Meijer CJ, Walboomers JM, Field JK. Prevalence of mucosotropic human papillomaviruses in squamous-cell carcinoma of the head and neck. Int J Cancer 1996;66:464–9.
- Stressgen Biotechnologies Corp. Data on File, 2000.
- Von Knebel Doeberitz M, Rittmuller C, zur Hausen H, Durst M. Inhibition of tumorigenicity of cervical cancer cells in nude mice by HPV E6–E7 anti-sense RNA. Int J Cancer 1992;51:831–4.
- Zur Hausen, H., 1991. Human papillomaviruses in the pathogenesis of anogenital cancer. Virology 184, 9–13.
Article Information
Sr No: 2
Page No: 51-55
Size:
Download:
Cited By:
Language: English
Licence: IJW
Authors: Shainda Laeeq*, Dr. Suman Rao Vihari, Istafa Husain Khan
Authors Address: *Lecturer, Department of Pharmacology, Maharana Pratap Dental College, Mandhana, Kanpur.
Email: shaindalaeeq786@gmail.com
Published: 14 November, 2014