


Update on perinatal and pediatric vitamin D
Update on perinatal and pediatric vitamin D
- V. K. TANDON*
*Senior consultant, Chhatrapati Shahu ji Maharaj University, Kanpur
Uttar Pradesh-208024, India
Mobile-9415043517
Correspondence to: email- vishnutandon.vt@gmail.com
ABSTRACT
Context: Vitamin D has emerged as a topic of great interest among researchers. Recent evidence indicates that today the world is facing vitamin D deficiency pandemic. Sensitizing pediatricians to widespread vitamin D deficiency in children and benefits accrued from it’s correction would go a long way as far as clinical practice and public health is concerned.
Evidence Acquisition: We performed a literature search using PubMed/medline, EMBASE and Science Direct databases indexed under the Medical Subject Heading (MeSH) terms; “Vitamin D OR Vitamin D deficiency” combined with the terms “children” OR “pediatric” OR “child health”. The literature search was limited to articles in last 35 years and written in the English language. All articles having direct relevance to the present review were searched. Reference lists of all articles were also reviewed. Emphasis was placed on pediatric literature, although sentinel adult studies relevant to this article have been included. Latest editions of standard texts were also searched.
Results: Vitamin D deficiency is highly prevalent throughout the world including India. Though some evidence suggests a role of hypovitaminosis D in pathophysiology of many clinical situations other than rickets and osteomalacia like autoimmune diseases, cardiovascular diseases, infections, cancers, fetal health, and exercise performance, some authorities feel there is a lack of unequivocal evidence in favour of nonskeletal health benefits of vitamin D.
Conclusions: Widespread subclinical and pre-rachitic vitamin D deficiency in children should be diagnosed by serum 25(OH)D levels and these levels should be maintained above 20 ng/mL to obtain optimal health benefits. There is a need for large randomized clinical trials to investigate the nonskeletal benefits of vitamin D deficiency.
Key words: Vitamin D, Deficiency, Child health, Hypovitaminosis D, Rickets
Till few decades ago, vitamin D was thought of only in relation to bone health and calcium homeostasis. Now, medical and nonmedical fraternities across the world are getting increasingly curious and realizing the potential role vitamin D plays in health and disease. There had been a rise in the rate of publication of peer reviewed articles on vitamin D in PubMed from about 100 articles per year in 1975 to >1400 in 20071. Time magazine has reported vitamin D as one of the top 10 medical breakthroughs of 20072.
New York Times has claimed vitamin D as a potential new miracle drug3. It stands at the frontline of current scientific endeavors, being a topic of greatest interest to medical researchers all over the globe. A growing body of evidence, implicating hypovitaminosis D as a risk factor for many diseases right from conception throughout lifespan, implies that awareness and management of widespread vitamin D deficiency may fetch profound future health benefits.
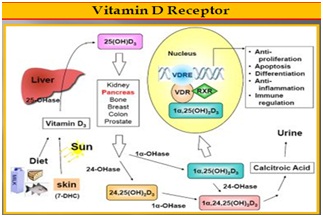
Vitamin D is not a true vitamin, because individuals with adequate exposure to sunlight do not require any dietary supplements. It is a steroid hormone acting on specific cell receptor to regulate various tissue processes. Vitamin D2 (ergocalciferol), obtained from influence of ultraviolet B radiations (UVR) on plants and yeast and vitamin D3 (cholecalciferol), produced in skin by UVR (UV-B and not UV-A) are the two main forms of vitamin D. Both forms are metabolised similarly in the body, first by hepatic 25 hydroxylation into inactive but stable 25(OH)D (Calcidiol) and then by renal 1 hydroxylation into active but unstable 1,25(OH)2D (Calcitriol). Calcitriol exerts it’s effects by binding to vitamin D receptor (VDR), which belongs to the family of nuclear hormone receptors. In vitamin D sufficient state, net intestinal calcium absorption is between 30-80%, which goes down to 10-15% in vitamin D deficient state4. Resultant Hypocalcemia stimulates parathyroid hormone (PTH) secretion leading to increased calcium reabsorption and phosphorus loss in renal tubules and increased synthesis of 1,25 (OH)2-D. Decreased calcium phosphorus product leads to reduced bone mineralisation causing rickets in growing bones and osteomalacia in mature bones. Vitamin D is measured in various units; 400 IU equals 10 μg or 26 nmol.
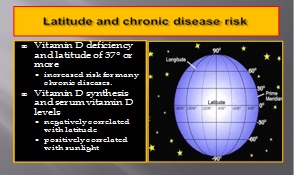
Recent data indicates that vitamin D deficiency is pandemic, even the healthy and the young are not spared. High prevalence rates are reported in otherwise healthy infants, children and adolescents5-8, and also from diverse countries around the world including India9,10.
DEFICIENCY OF ‘SUNSHINE VITAMIN’ IN SUNNY COUNTRIES
Adapted from Vitamin D and Health by, Heli J. Roy, PhD, MBA, RD, Pennington Biomedical Research Center
Major source of vitamin D for our body is cutaneous synthesis through the effect of UVR on 7-dehydrocholesterol because dietary source through fatty fishes, organ meat,
egg yolk, cod liver oil and milk products does not contribute significantly as these are not consumed in sufficient quantities by children. Thus fortifying foods with vitamin D
remains the only alternative in case cutaneous synthesis is inadequate. It is surprising and disturbing to note that hypovitaminosis D is highly prevalent even in areas with
adequate sunshine10-15. Sensitizing pediatricians and health policy makers to this fact has important implications on child health, as widely held notion that vitamin D
supplementation is not necessary in sun replete areas is preventing policy makers from coming out with definite guidelines regarding vitamin D requirements. There are
many factors which can explain this paradox of hypovitaminosis D inspite of abundant sunshine like duration and timing of sun exposure, amount of skin exposed,
atmospheric pollution, skin pigmentation, sunscreen use, dietary and genetic factors4,11,16. Modern day life style changes have significantly reduced the total duration of
sun exposure in children. UV-B, having shorter wavelength, tend to scatter earlier or later in the day and hence cutaneous vitamin D synthesis is maximum between 10
AM to 3 PM, the time when most of the children are either in school or indoors. Exposure of only face, hands and arms due to clothing versus whole body is associated
with marked differences in vitamin D synthesis17. Cloud cover, increasing water vapour and industrial pollution can reduce the amount of UV-B that reaches the earth’s
surface18. Epidermal melanin (a natural sunscreen) on one hand reduces the risk of skin cancer induced by UVR but on the other hand, reduces cutaneous vitamin D
synthesis. An asian Indian would require 3 times the sun exposure than light-skinned person to produce equivalent amount of vitamin D17. It is interesting to note that
women of all population have lighter skin than men, presumably because of increased vitamin D needs during pregnancy and lactation19. Sunscreens block UV-B more
than UV-A and sunscreens with sun protection factor (SPF) of 8 and 15 will decrease vitamin Dsynthetic capacity by 95% and 98%,respectively20. Dietary factors like
very low calcium intake and high fibre diet may deplete vitamin D stores21. Genetic factors like increased 25(OH)D-24- hydroxylase (leading to degradation of vitaminD)
activity in South Asians21 are also among the various explanations of hypovitaminosis D in sunny countries. Given the facts that vitamin D crosses the placenta and poor
vitamin D content of breast milk even in vitamin D replete mothers, maternal vitamin D deficiency and exclusive breastfeeding without vitamin D supplements or adequate
sunlight exposure are important risk factors for vitamin D deficiency in infants.
CALCIOTROPIC TO PLEIOTROPIC ROLE
Calciotropic effects of vitamin D on intestine, bone and kidney are known to medical science since ages. Recent and mounting evidence suggests that this secosteroid
hormone plays pleiotropic role influencing numerous bodily processes in addition to calcium metabolism. Vitamin D pleiotropism concept has it’s origin in two discoveries
22, 23. The first is discovery of VDRs in non-osseous tissues. To date VDRs are found in more than 30 tissues including heart, intestine, liver, kidney, lungs, brain, muscle,
skin, pancreas and various immune cells. The second is the discovery of enzyme CYP27B1 (capable of converting 25(OH)D into 1,25(OH)2D) in various tissues throughout the body. These findings suggest local autocrine
and paracrine role for vitamin D in addition to it’s role as an endocrine hormone24. The nonskeletal autocrine effects of vitamin D are essentially different from it’s skeletal
effects in that the former operate outside the tight feedback-controlled endocrine loop (independent of regulation by serum calcium, phosphorus and PTH levels)23,25 and
are more substrate dependent26. This observation gave birth to the concept of maintaining an adequate blood level of vitamin D for regulating it’s various nonosseous
functions. This autocrine pathway of vitamin D, responsible for it’s nonskeletal effects, has three key features22 : (a) The bulk of the daily metabolic utilization of vitamin D
is by way of the peripheral autocrine pathway; (b) autocrine action always results in expression of the 24-hydroxylase leading to degradation of locally synthesized
calcitriol after it’s action is over, so that no calcitrol which is locally produced enters the circulation; and (c) local concentration of calcitriol required to support various
tissue responses are higher than typical serum concentrations of calcitriol. When bound to the vitamin D receptor, calcitriol seems to be just the right key to open up the
locked stores of DNA information, allowing cells to produce proteins needed for tissue specific responses22. As amount of calcitriol produced locally is substrate
dependent, optimal serum level of 25(OH)D is crucial in maintaining ability of the cell to respond to pathological stimuli.
BEYOND BONES AND CALCIUM
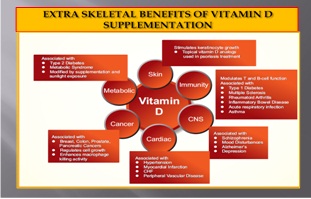
Apart from its conventionally understood actions on bone health and calcium homeostasis, vitamin D is believed to have effect on body’s endocrine system, immune
system, cardiovascular system, neuropsychological functioning, neuromuscular performance and is also believed to act as a potent antioxidant protecting against free
radical damage, as well as being an inducer of cellular differentiation, protecting against carcinogenesis20,24. The term “vitamin D deficiency” does not necessarily connote
clinically explicit disease, rather it means an increase in risk for certain diseases and that also explains the seeming paradox that individuals who are ostensibly healthy
today may nevertheless be “deficient”22. As these diseases are multifactorial, vitamin D deficiency, rather than being directly causal, acts by hampering the ability of
tissues to deal adequately with physiological and pathological stimuli and though these diseases will continue to occur in presence of optimum vitamin D status, their risk
will be lowered22.Though some studies suggest the potential role of vitamin D in immunological diseases (Type I diabetes, asthma, multiple sclerosis, rheumatoid arthritis,
inflammatory bowel diseases) through reduced activation of acquired immune system27-32, various cancers through antiproliferative and prodifferentiating actions26,33,34,
infectious diseases through enhancement of the innate immune system and production of antimicrobial peptide cathelicidin or LL-3723,35-40, fetal health16,41 and
cardiovascular diseases, type II diabetes, obesity and hypertension24,42; large, randomized, controlled trials are needed to establish nonskeletal role of vtamin D unequivocally.
PRERACHITIC, SUBCLINICAL VITAMIN D DEFICIENCY
Vitamin D deficiency can be easily diagnosed in presence of clinical features of rickets. But rickets is an extreme form of vitamin D deficiency and represents the tip of
vitamin D deficiency iceberg25. Improved understanding of the detrimental effects of insufficient vitamin D before the appearance of rickets led to a growing interest in these
lesser degrees of vitamin D deficiency43 and diagnosing this prerachitic, subclinical vitamin D deficiency is important for nonskeletal health benefits. Serum 25 (OH) D
level is the best available biomarker for the diagnosis of vitamin D deficiency. It should be emphasised here that serum level of 1,25(OH)2D is not a good indicator of
vitamin D deficiency because (i) subtle hypocalcemia
causes PTH elevations leading to increased 1-a-hydroxylase activity resulting into normal or elevated 1,25(OH)2D in face of vitamin D deficiency, (ii) circulating
concentrations of 1,25(OH)2D are 100 to 1000 fold less abundant than 25 (OH) D(4), (iii) half life of 1,25(OH)2D is only 4 hours as against 3 to 4 weeks in case of 25 (OH) D and (iv) 25 (OH) D is the storage form of vitamin D.
CHANGING DEFINITIONS OF VITAMIN D STATUS
Based on the study of biomarkers like PTH and intestinal calcium absorption and functional health outcomes, there has been a dramatic change in the definition of vitamin
D deficiency over last few years. Institute of Medicine (IOM) and the American Academy of Pediatrics (AAP) in 1997 defined vitamin D deficiency in infants and children as
a serum 25 (OH) D level below 11 ng/mL44,45 but level below 20 ng/mL are now considered insufficient4. Table-1 shows the classification of vitamin D status based on
serum 25 (OH) D level4. IOM recently published a review46 on dietary reference intakes for calcium and vitamin D. This review expressed that, as studies regarding
nonskeletal health benefits provided mixed and inconclusive results, as yet there is insufficient evidence to recommend higher levels of serum 25(OH)D. It feels that
benefits for most in the population is associated with levels of approximately 20 ng/mL and use of higher cutoffs would artificially increase the estimates of prevalence of
vitamin D deficiency. This review has taken skeletal health as the basis for Dietary Reference Intakes (DRI). There is an urgent need to follow these current definitions of
vitamin D status, as pediatricians (and obstetricians) are blamed for being a little slow to address the suboptimal vitamin D status of their patients47.
Table 1: Vitamin D Status in Relation to 25(OH) Level
Vitamin D status Serum 25(OH)D level (ng/mL)
Severe deficiency £5
Deficiency £15
Insufficiency 15-20
Sufficiency 20-100
Excess >100
Intoxication >150 .
Adapted from Misra, et al.[4]
|
Table 2: Vitamin D doses based on serum 25(OH)D levels
Serum 25(OH)D Low dose Vitamin D High doseVitamin D Total duration of (ng/mL) therapy (IU/day) therapy (IU) therapy (months)
< 5 8000 50,000/week × 4weeks 50,000/fortnight × 8 weeks 3 5-15 4000 50,000/fortnight 3 16-30 2000 50,000/month 3 Adapted from Holick [50].
|
REVISED GUIDELINES FOR VITAMIN D RDA
There appears to be a discrepancy between vitamin D RDA (Recommended Dietary Allowance) based on recent research and current practice48. In 2003, the AAP
Committee on Nutrition and section on Breastfeeding advocated 200 IU per day of vitamin D intake for children of all ages49,50 but this amount was deemed to prevent the
worst outcome of vitamin D deficiency i.e. rickets. But now the recommendation is 400 IU per day for all infants, children and adolescents4,49 till they are not getting this
amount from alternative sources. It is likely that higher doses may be needed for dark skinned and preterm infants4. Supplementation trials in infants and children have
shown that 400-1000 IU per day are needed to achieve serum level of 30 ng/mL50. For children and adolescents (1 to 18 years of age), IOM46 has specified estimated
average requirements (EARs) and RDAs on the basis of serum 25(OH)D levels of 16 and 20 ng/mL, respectively. EAR and RDA for vitamin D, as per IOM review, are 400
IU/day
and 600 IU/day respectively, while tolerable upper level of intake are 1000 IU/day for infants <6 months old, 1500 IU/day for 6-12 months old, 2500 IU/day for 1-3 years old,
3000 IU/day for 4-8 years old and 4000 IU/day for 9 years and above including pregnant and lactating mothers. The RDA estimates here have been made considering the
minimal skin synthesis of vitamin D.
THERAPEUTICS OF VITAMIN D DEFICIENCY
Either D2 or D3 can be used for the treatment of hypovitaminosis D but D2 is not available in India. 1 mcg of either provides 40 IU,although D3 raises serum 25(OH)D
levels upto three-fold higher than D251. It is important to note that 1-alphacalcidol should not be used for the treatment of vitamin D deficiency47. Vitamin D given in daily
doses of 1000-10,000 IU (depending on the age of the child) for a period of 3 months will normalise serum 25(OH)D and replenish stores4. Doses recommended are 1000
IU/day for neonates, 1000- 5000 IU/day for infants (1-12 months old) and >5000 IU/day for children >1 year old4,52. If noncompliance is an issue, administration of high
doses 1,00,000-6,00,000 IU over 1-5 days is an alternative for >1 month old53. In teenagers and adults, 50,000 IU orally once a week for 8 weeks has been successfully
used25. Vitamin D doses, based on serum 25(OH)D levels, are used in case of children with kidney diseases or other chronic diseases as shown in Table 251. It is
estimated that each 100 IU of additional daily oral vitamin D intake produces an elevation of serum 25(OH)D of approximately 1 ng/mL and hence a patient having 10
ng/mL would need approximately 2000 IU/day to bring serum level of 25(OH)Dup to 30 ng/mL54, though it should be remembered that individual response to standard
doses varies widely. Toxicity due to excess vitamin D is rare, but has been reported, generally with doses exceeding 10,000 IU/ day or single doses greater than 300,000
IU or withserum 25(OH)D levels of more than 100-150 ng/mL9. There is enough margin of safety between doses levels and those associated with toxicity. Calcium
supplementation is necessary with vitamin D therapy to prevent hypocalcemia of ‘hungry bone syndrome’ associated with remineralisation of bone matrix. Calcium is used
in the dose of 30-75 mg/kg/day of elemental calcium. Elemental calcium content of various calcium preparations are 9 mg/mL of calcium gluconate, 27 mg/mL of calcium
chloride, 40% of calcium carbonate, 6% of calcium glubionate and 39% of tribasic calcium phosphate. After correction of deficiency, maintainance dose of 400-1000
IU/day of vitamin D or high dose every 3 months is needed. Vitamin D supplementation (at least 400 IU and perhaps as high as 800-1000 IU/day) is appropriate throughout
life if sunlight exposure is limited55. Calcium supplements are not necessary after serum 25(OH)D levels are normalized.
CONCLUSION
The world is currently facing an unrecognized and untreated pandemic of vitamin D deficiency. Sensitising pediatricians to recognise and treat this pandemic would have great impact on child health in the 21st century. Vitamin D deficiency is common even in countries with abundant sunshine. As a part of it’s autocrine function, vitamin D has multiple non-skeletal effects and these depend solely on it’s optimal circulating levels. Though observational studies suggest that correction of vitamin D deficiency lowers the risk of many long latency diseases like cancers, autoimmune diseases and cardiovascular diseases, and it also decreases the risk of infectious diseases and improves fetal health, muscle function and exercise performance; we need large, randomized, controlled trials before any recommendation for it’s use is made in these diseases. Measurement of serum 25(OH)D level is the only way to diagnose subclinical, prerachitic vitamin D deficiency and recent evidence suggests maintaining it above 20 ng/mL for maximizing health benefits. Optimum doses of vitamin D should be used for prevention and treatment of vitamin D deficiency. We suggest ICMR should come out with definite guidelines regarding vitamin D RDA and health policy makers should take serious steps regarding food fortification with vitamin D.
REFERENCES
1. Norman AW. A vitamin D nutritional cornucopia: new insights concerning the serum 25-hydroxyvitamin D status of the US population. Am J Clin Nutr. 2008;88:1455-6.
2. Catherine G. Time Magazine 2007; Dec 9 [Online Edition].
3. Parker-Pope T. The miracle of vitamin D : sound science or hype? NY Times 2010; Feb 1. Available at http://well.blogs.nytimes.com/2010/ 02/01/the-miracle-of-vitamin-d-sound-science-or-hype/?_r=0
4. Misra M, Pacaud D, Petryk A, Collett-Solberg PF, Kappy M. Vitamin D deficiency in children and it’s management : Review of current knowledge and recommendations. Pediatrics 2008;122:398-417.
5. Holick MF. The vitamin D deficiency pandemic and consequences for nonskeletal health: mechanisms of action. Mol Aspects Med 2008; 29:361-8.
6. Gordon CM, DePeter KC, Feldman HA, Grace E, Emans SJ. Prevalence of vitamin D deficiency among healthy adolescents. Arch Pediatr Adolesc Med 2004;
158:531-7.
7. Gordon CM, Feldman H, Sinclair L, Williams A, Cox J. Prevalence of vitamin D deficiency among healthy infants and toddlers. Arch Pediatr Adolesc Med 2008; 162:505-12.
8. Lee JM, Smith JR, Philipp BL, Chen TC, Mathieu J, Holick MF. Vitamin D deficiency in a healthy group of mothers and newborn infants. Clin Pediatr 2007;46:42-4.
9. Huh SY, Gordon CM. Vitamin D deficiency in children and adolescents: Epidemiology, impact and treatment. Rev Endocr Metab Disord 2008;9:161-70.
10. Marwaha RK, Tandon N, Agrawal N, Puri S, Agrawal R, Singh S, et al. Impact of two regimens of vitamin D supplementation on calcium-vitamin D-PTH axis of school girls of Delhi. Indian Pediatr 2010;47:761-9.
11. Khadilkar AV. Vitamin D Deficiency in Indian adolescents. Indian Pediatr. 2010; 47:755-6.
12. Puri S, Marwaha RK, Agrawal N, Tandon N, Agrawal R, Grewal K, et al. Vitamin D status of apparently healthy schoolgirls from two different socioeconomic strata in Delhi: relation to nutrition and lifestyle. Br J Nutr 2008;99:876-82.
13. Marwaha RK, Tandon N, Reddy DHK, Agrawal R, Singh R, Sawhney RC, et al. Vitamin D and bone mineral density status of healthy school children in northern India. Am J Clin Nutr 2005;82:477-82.
14. Gannage-Yared MH, Chemali R, Yaacoub N, Halaby G. Hypovitaminosis D in a sunny country: relation to lifestyle and bone markers. J Bone Miner Res 2000;15: 1856-62.
15. El-Hajj Fuleihan G, Deeb M. Hypovitaminosis D in a sunny country. N Engl J Med 1999;340:1840-18401.
16. Wagner CL, Greer FR. Prevention of rickets and vitamin D deficiency in infants, children and adolescents. Pediatrics 2008;122:1142-52.
17. Hollis BW. Circulating 25-hydroxyvitamin D levels indicative of vitamin D sufficiency: implications for establishing a new effective dietary intake recommendation for vitamin D. J Nutr 2005;135:317-22.
18. Agarwal KS, Mughal MZ, Upadhyay P, Berry JL, Mawer EB, Puliyel JM. The impact of atmospheric pollution on vitamin D status of infants and toddlers in Delhi, India. Arch Dis Child 2002;87:111-3.
19. Glimcher ME, Garcia RI, Szabo G. Organ culture of mammalian skin and the effects of ultraviolet light and testosterone on melanocyte morphology and function. J Exp Zool 1978;204:229-37.
20. Holick MF. Sunlight and vitamin D for bone health and prevention of autoimmune diseases, cancers and cardiovascular disease. Am J Clin Nutr 2004;80:1678S-88S.
21. Khadilkar A, Das G, Sayyad M, Sanwalka N, Bhandari D, Khadilkar V, et al. Low calcium intake and hypovitaminosis D in adolescent girls. Arch Dis Child 2007;92:1045.
22. Heaney RP. Vitamin D in health and disease. Clin J Am Soc Nephrol 2008;3:1535-41.
23. Chesney RW. Vitamin D and the magic mountain: The anti-infectious role of the vitamin. J Pediatr 2010;156:698-703.
24. Bartoszewska M, Kamboj M, Patel DR. Vitamin D, muscle function and exercise performance. Pediatr Clin North Am 2010;57:849- 61.
25. Holick MF. Vitamin D deficiency. N Engl J Med 2007;357:266-81.
26. Bikle D. Nonclassic actions of vitamin D. J Clin Endocrinol Metab 2009;94:26-34.
27. Hypponen E, Laara E, Reunanen A, Jarvelin MR, Virtanen SM. Intake of vitamin D and risk of type I diabetes: a birthcohort study. Lancet 2001; 358:1500-3.
28. Camargo CA Jr, Rifas-Shiman SL, Litonjua AA, Rich- Edwards JW, Weiss ST, Gold DR, et al. Maternal intake of vitamin D during pregnancy and risk of recurrent wheeze in children at 3 y of age. Am J Clin Nutr 2007;85:788-95.
29. Litonjua AA. Childhood asthma may be a consequence of vitamin D deficiency. Curr Opin Allergy Clin Immunol 2009;9: 202-7.
30. Munger KL, Levin LI, Hollis BW, Howard NS, Ascherio A. Serum 25 hydroxyvitamin D levels and risk of multiple sclerosis. JAMA 2006; 296:2832-8.
31. Merlino LA, Curtis J, Mikuls TR, Cerhan JR, Criswell LA, Saag KG. Vitamin D intake is inversely associated with rheumatoid arthritis: results from the Iowa Women’s Health Study. Arthritis Rheum 2004;50:72-7.
32. Cantorna MT, Munsick C, Bemiss C, Mahon BD. 1,25-Dihydroxycholecalciferol prevents and ameliorates symptoms of experimental murine inflammatory bowel disease J Nutr. 2000;130: 2648-52.
33. Garland CF, Garland FC, Gorham ED, Lipkin M, Newmark H, Mohr SB, et al. The role of vitamin D in cancer prevention. Am J Public Health 2006; 96:252-61.
34. Lappe JM, Travers-Gustafson D, Davies KM, Recker RR, Heaney RP. Vitamin D and calcium supplementation reduces cancer risk: results of a randomized trial. Am J Clin Nutr 2007;85:1586-91.
35. Wilkinson RJ, Llewelyn M, Toossi Z, Patel P, Pasvol G, Lalvani A et al. Influence of vitamin D deficiency and vitamin D receptor polymorphisms on tuberculosis among Gujarati Asians in west London: a case-control study. Lancet 2000;355: 618-21.
36. Martineau AR, Wilkinson RJ, Wilkinson KA, Newton SM, Kampmann B, Hall BM, et al. A single dose of vitamin D enhances immunity to Mycobacteria. Am J Respir Crit Care Med 2007; 176:208-13.
37. Urashima M, Segawa T, Okazaki M, Kurihara M, Wada Y, Ida H. Randomized trial of vitamin D supplementation to prevent seasonal influenza A in schoolchildren. Am J Clin Nutr 2010;91:1255-60.
38. Muhe I, Lulseged S, Mason KE, Simoes EA. Case-control study of the role of nutritional rickets in the risk of developing pneumonia in Ethiopian children. Lancet1997;349:1801-4.
39. Karatekin G, Kaya A, Salihog lu O, Balci H, Nuhog lu A. Association of subclinical vitamin D deficiency in newborns with acute lower respiratory infection and their mothers. Eur J Clin Nutr 2009;63:473-7.
40. Wayse V, Yousafzai A, Mogale K, Filteau S. Association of subclinical vitamin D deficiency with severe acute lower respiratory infection in Indian children under 5 year. Eur J Clin Nutr 2004;58:563-7.
41. Mannion C, Gray-Donald K, Koski K. Association of low intake of milk and vitamin D during pregnancy with decreased birth weight. CMAJ 2006;174:1273-7.
42. Perez-Lopez FR. Vitamin D and it’s implications for musculoskeletal health in women: an update. Maturitas 2007;58:117-37.
43. Mansbach JM, Ginde AA, Camargo Jr CA. Serum 25- Hydroxyvitamin D levels among US children aged 1 to 11 years: Do children need more vitamin D?Pediatrics 2009;124:1404-10.
44. Standing Committee on the Scientific Evaluation of Dietary Reference Intakes Institute of Medicine. Dietary Reference Intakes for Calcium, Phosphorus, Magnesium, Vitamin D, and Fluoride. Washington, DC: National Academy; 1997.
45. Gartner LM, Greer FR. Prevention of rickets and vitamin D deficiency: new guidelines for vitamin D intake. Pediatrics 2003;111:908-10.
46. Ross AC, Taylor CL, Yaktine AL, Del Valle HB. Dietary Reference Intakes for Calcium and Vitamin D. Committee to Review Dietary reference Intakes for Vitamin D and calcium. Food and Nutrition Board, Institute of Medicine. The National Academies Press, Washington D.C.; 2010.
47. Cheetham D. Vitamin D supplementation – Still in it’s infancy. Indian Pediatr 2010;47:573-4.
48. Canadian Pediatric Society. Vitamin Dsupplementation: recommendations for Canadian mothers and infants. Paediatr Child Health 2007;12:583-9.
49. Calikoglu AS, Davenport ML. Prophylactic vitamin D supplementation. Endocr Dev `2003;6:233-58.
50. Holick MF. Resurrection of vitamin D deficiency and rickets. J Clin Invest 2006;116:2062-72.
51. Buck MI. Prevention and management of vitamin D deficiency in children: Part II. Vitamin Dsupplementation. Alim Pharm Therap 2009;30: 508-15.
52. Munns C, Zacharin MR, Rodda CP, Batch J, Morley R, Cranswick N, et al. Prevention and treatment of infants and childhood vitamin D deficiency in Australia and New Zealand: a consensus statement. Med J Aust 2006;185:268-72.
53. Hochberg Z, Bereket A, Davenport M, delemarre-Van de wall HA, Schepper JD, Levine MA, et al. Consensus development for the supplementation of vitamin D in childhood and adolescence. Horm Res 2002;58:39-51.
54. Heaney RP, Davies KM, Chen TC, Holick MF, Barger-Lux MJ. Human serum 25-Hydroxy-cholecalciferol response to extended oral dosing with cholecalciferol. Am J Clin Nutr 2003;77:204-10.
55. Root AW, Diamond FB. Disorders of mineral homeostasis in the newborn, child and adolescent. In: Sperling MA,Eds. Pediatric Endocrinology. Philadelphia PA: 3rd Ed, Saunders Elsevier; 2008. p.686-769.