


Reliability and responsiveness of lysholm knee scoring scale and knee outcome survey activity of daily living scale (ADLS) for patients with anterior cruciate ligament reconstruction
Research Article
Reliability and responsiveness of lysholm knee scoring scale and knee outcome survey activity of daily living scale (ADLS) for patients with anterior cruciate ligament reconstruction
Sneha Narang Gandhi*1, Suvarna Shyam Ganvir2
1 Guest Assistant Professor, University Institute of Health Sciences, CSJM University, Kanpur.
Consultant, The Spastic Centre, Kanpur.
111A/131, Ashok Nagar, Behind Kanha continental, Kanpur, Mobile no - 7897957777
2 Professor, PDVVPF’S College of physiotherapy, Ahmednagar , Mobile no - 9372910683
ABSTRACT
Objective: To Find out the Reliability and Responsiveness of Lysholm Knee scoring scale and Knee Outcome Survey Activity of Daily Living Scale in patients with Anterior Cruciate Ligament Reconstruction .
Study design : Prospective and Observational study with Repeated Measures
Method: 30 Patients were included. The study included an initial assessment and a follow up assessment. On the initial assessment (24 to 48 hrs) after reconstruction, with the help of Lysholm Knee Scoring Scale and Activity of Daily Living Scale, score were recorded. Second assessment was done after one day in order to estimate the test retest reliability and the follow assessment was done every month for consecutively 3 months .Data was analysed using spearman correlation coefficient and standard error of measurement.
Results: Both the scales was statistically significant .but there was a higher value for activity of daily living scale (0.97 to 0.99) as compared to Lysholm knee scoring scale (0.78 to 0.88) and Activity of daily living scale had higher standard error of measurement (1.11) than Lysholm knee scoring scale
Conclusion: The results obtained from the study shows that Activity of Daily Living Scale appears more useful instrument for measurement of functional limitations.
Key words: Scales, Anterior cruciate ligament, functional measurements
INTRODUCTION
Anterior cruciate ligament injury is common in knee joint, accounting for 40% of sports injury1. Sports injury is common, ranking the second highest (21%) in terms of
cause of injury2 and leading to long term disabilities and handicaps especially in patients with knee injuries3.Among all sport related knee injuries, one fifth (20%) consist
of anterior cruciate ligament injury, the most traumatized structure4. Anterior Cruciate Ligament ruptures results in knee instability5, prohibits the athlete from going back
to sports and resulting in early retirement6.
Anterior cruciate is a font crossing ligament attaching the femur to tibia through the knee; this ligament keeps the knee from hyperextension or being displaced back from
femur7. The primary function of anterior cruciate ligament is to control anterior translation of the tibia. The Anterior Cruciate Ligament is also a secondary restraint to tibial
rotation as well as varus or valgus stress8,9 This ligament ruptures causes joint laxity, especially on rotational movement and often causes disability to practice sports
and joint wear off10.
The Anterior cruciate ligament is rather large ligament that can withstand 500 lb (20kg) of pressure. If it is torn or becomes detached it remains that way and surgery is
indicated7. In most severe cases, graft to the ligament is necessary to reattach it to the bone. The surgery can use tissue from the patient called as autograft7.
The prognosis for a partially torn Anterior cruciate ligament instability symptoms is sometimes favourable with the recovery and rehabilitation period usually at least 3
months11.
In United States there are between 10,000 and 20,000 ACL ruptures per year, with an annual incidence in the general population of approximately 1 in 3500, although the
actual incidence must be higher12, 13. Women are nearly three times more likely to have anterior cruciate ligament injuries than men. This is due to difference in hormone
levels or ligament strength and stiffness, neuromuscular control, lower limb biomechanics ligament strength and fatigue14.There are several areas of controversy regarding
the management of anterior cruciate ligament injuries. These include the relative merits of conservative versus surgical management15Whether or not the patient performs
pivoting sports
A minor anterior cruciate ligament injury is like any other soft tissue injury and should be treated accordingly. This involves the application of RICE -R. Rest, ice, compression, elevation and obtaining a R -referral for appropriate medical treatment16.There is always a chance of developing stiff knee after surgery and loss of motion,
especially loss of extension. Loss of knee extension has been shown to result in a limp, quadriceps muscle weakness and anterior knee pain17.
Preoperative Rehabilitation Phase17
Goals: Control pain and swelling
* Restore normal range of motion
* Develop muscle strength sufficient for normal gait and ADL
* Mentally prepare the patient for surgery
Restore normal range of motion
Full extension is obtained
Bending (Flexion) is obtained
Heel slides are used to gain final degrees of flexion.
In later stages of rehabilitation, do heel slides by grasping the leg with both hands and pulling the heel toward the buttocks.
Develop muscle strength
Postoperative Days 1 – 717
IT IS EXTREMELY IMPORTANT THAT PATIENT WORK ON EXTENSION IMMEDIATELY.
Goals:
* Control pain and swelling
* Care for the knee and dressing
* Early range of motion exercises
* Achieve and maintain full passive extension
* Prevent disuse atrophy of the quadriceps muscles
* Gait training
Postoperative Days 8 – 1017
Maintain full extension
Return to work
1) Schedule an office follow-up.
2) After 3 weeks, patient may apply vitamin E oil or another emollient to the incisions, as this will improve their appearance.
3) The appearance of patient incision can be improved further by avoiding the direct sunlight for one year. When exposed to the sun the incisions can be covered with a bandage.
Achieve full Extension
Develop Muscular Control
Control Pain and Swelling
Postoperative Weeks 3 – 417
Goals:
* To achieve full range of motion
* To gain the strength of muscles through exercise
Expected range of motion is from full extension to 100 – 120 degrees of flexion.
Postoperative Weeks 4 – 617
Goals:
* To achieve 125 degrees of flexion pushing toward full flexion
* strengthening of the muscle should continue.
Postoperative Weeks 6 – 1217
By week 6, patient range of motion should be full extension and at least 135 degrees of flexion.
Goals:
* 135 degree of flexion
* Maintainence of strength
Postoperative Weeks 12 – 2017
Goals:
* Maintain strength
* Jogging and light running should be taught to the patient
* Determine need for ACL functional brace
24 Weeks Postoperative (6 months) 17
Goals: * Return to sports
To return to sports patient should have: 17
Disablement after anterior cruciate ligament reconstruction can be categorised according to International Classification of the Impairment, Disability and Handicap as
either physical impairment or disabilities related to injury18, 19
Impairments after Anterior ligament injury are anatomic (anterior or displacement of tibia relative to femur) and physiologic (range of motion, muscle performance, pain) 20
Disabilities outcome related to Anterior cruciate ligament injuries has traditionally been measured with questionnaire such as Lysholm Knee Scoring Scale, Activity Of
Daily Living Scale and Functional knee test21,22
Studies have shown a moderate correlation between quadriceps muscle performance (impairment) and lower limb performance during functional knee test (disability)23.
Impairment was measured by various means:
Goniometer to record active and passive ROM. Extension deficit was a major impairment after the ACL reconstruction24, 25.
Measures of functional limitations and disabilities include performed based clinical assessment – such as one leg hop test and patient reported assessment 26.
The difference with use of performance based measures of function in the clinical setting and dearth of normative data for interpretations have it. The practitioner to
consider alternatives such as patient reported measure of function also26.
There are many rating scale available to measure outcome in patients with disorders of the knee28.
Specific patient reported measures of functions of the knee include Lysholm Knee Scale29, Cincinnati Knee Scale30, Western Ontario and Mc Master Universities
Osteoarthritis Index (WOMAC)31, Activity of Daily Living Scale, patellofemoral joint evaluation scale.
The available patient reported measure of function of the knee were developed for specific pathological conditions such as OA and injuries of ligament29, 30, 31.
The majority of instruments were developed, 8 instruments were evaluated in patients with range of knee problems27.
Modified Lysholm Scale is an 8 item questionnaire originally designed to evaluate patients after knee ligament surgery28. The scale is scored on a 100 point scale, with
25 points attributed to knee stability, 25 to pain, 15 to locking, 10 each to swelling and stair climbing and 5 to each limp, use of a support and squatting. It has adequate
test retest reliability and good construct validity 28.
The American academy of orthopaedics surgeons (AAOS) sports knee rating scale was included in the musculoskeletal outcomes data evaluation and management
system (MODEMS) for athletic patients with disorder’s of the knee28
The activity of daily living scale of the knee outcome survey was published with the evaluation of its reliability, validity and responsiveness. This scale was developed on
the foundation of the relevance of the instrument and the clinical input28.
The single assessment numeric evaluation (SANE) was devised to evaluate college age patients following ACL reconstruction. The single assessment numeric evaluation
asks the patient how they would rate their knee, from zero to 100, with 100 being normal28.
The development of knee injury and osteoarthritis outcome score (KOOS) was the outcome of the feedback from the patients who were subjected to remote meniscal surgeries, and was found to be satisfactory on a sample size of 21 patients with anterior cruciate ligament reconstruction, through five separate scores based on pain,
symptoms, daily activity, sports and recreation and knee related issues 28
The quality of life outcome measure for chronic ACL deficiency was developed by Mohatadi.
Since outcome measures forms the important part of any research study as it is necessary that these outcome measures should have sound psychometric properties, it is the need of time to evaluate & establish the effectiveness of them. This study is an attempt to re-establish the basic qualities of some not so extensively studied scales used in the rehabilitation of patients with ACL injury.
Hence the purpose of the study is to find out the reliability and responsiveness of Lysholm Knee Scoring Scale and Knee Outcome Survey Activity of Daily Living Scale in patients with anterior cruciate ligament reconstruction
MATERIAL AND METHODS
Study Design
Prospective and observational study with repeated measures of patients with anterior cruciate ligament reconstruction, consisting of scales to measure functional abilities of the patient.
Study Setting
A 950 bedded tertiary care teaching hospital (Jawaharlal Nehru Medical College & Hospital, Wardha) with well equipped medical and surgical intensive care unit and a musculoskeletal department.
Sample and Sampling Method
Purposive sampling technique was used to select 30 patients with anterior cruciate ligament reconstruction.
Inclusion criteria
Exclusion criteria
ALTERNATE HYPOTHESIS- Lysholm Knee Scoring Scale and Knee Outcome Survey Activity of Daily Living Scale are reliable and responsive in Anterior Cruciate Ligament Reconstruction patients.
NULL HYPOTHESIS- Lysholm Knee Scoring Scale and Knee Outcome Survey Activity of Daily Living Scale are not reliable and responsive in anterior cruciate ligament reconstruction patients.
RESEARCH HYPOTHESIS – Does these two scales are reliable and responsive in patients with anterior cruciate ligament reconstruction?
Methodology
The synopsis of the study was submitted to the Institutional Ethical Committee (IEC) for approval. After obtaining the approval patients were taken for the study based on the inclusion and exclusion criteria. The purpose of the study was explained to the patients and they were informed about their right to opt out of the study anytime during the course of the study without giving reasons for doing so. A signed informed consent (Vernacular language) was obtained from all the patients who willingly volunteered for the study.
Initially patients were managed in the orthopaedics ward and in musculoskeletal department after reconstruction. The treatment approach were designed to meet the individuals need of the patients ,all the patients were asked to come for follow up with the treating therapist regularly every 15 days after their discharge from the orthopaedics department .
The assessment tool used in our study included Lysholm Knee Scoring Scale and Knee Outome -Activity of Daily Living Scale. Both of these are well established and with reliable measures.
The study included an initial assessment and a follow up assessment. On the initial assessment (24 to 48 hrs)after reconstruction , with the help of Lysholm Knee Scoring Scale and Knee Outcome Survey – Activity Of Daily Living Scale , scores were recorded .Second assessment was done after one day in order to examine test retest reliability and then follow up assessment was done every month for consecutively 3 months .The patients were interviewed about their performance on the scales, that is the Lysholm Knee Scoring Scale and Knee Outcome Survey Activity Of Daily Living Scale , the scores were recorded as the outcome measures .
Data Collection
The study conducted from December 2009 to September 2010 a prospective and observational study with repeated measures was carried out in patients with anterior cruciate ligament reconstruction as per the inclusion and exclusion criteria and data was collected and was subjected to appropriate statistical analysis .
Data Analysis
Data from all patients were entered into a computer data base analyzer with SPSS statistical package (version 14.0). Intra class correlation coefficient (ICC) was used to estimate test retest reliability. Reliability of both the scales was also measured using standard error of measurement (SEM). Spearman correlation coefficient was used to examine the relationship between the prognostic rating and change in the following functional status score at monthly interval for 3 months.
OBSERVATIONS AND RESULTS
Table 1: Age wise distribution of patients
|
Age Group(yrs) |
No. of patients |
Percentage (%) |
|
20-30 |
11 |
36.67 |
|
31-40 |
19 |
63.33 |
|
Total |
30 |
100.00 |
|
Mean |
33.56 yrs |
|
|
SD |
7.09 |
|

Graph 1: Age wise distribution of patients
Table 2: Comparison of Lysholm knee Scoring scale at 24-48 hrs, 1 day, 1 month, 2nd month and 3rd month
Descriptive Statistics
|
|
Mean |
N |
Std. Deviation |
Std. Error Mean |
|
24-48 hrs |
15.33 |
30 |
2.29 |
0.41 |
|
1day |
17.53 |
30 |
2.54 |
0.46 |
|
1 month |
46.83 |
30 |
2.76 |
0.50 |
|
2 month |
49.70 |
30 |
3.45 |
0.63 |
|
3 month |
70.83 |
30 |
8.27 |
1.51 |
Students paired t test
|
|
Paired Differences |
t |
df |
p-value |
||||
|
Mean |
Std. Deviation |
Std. Error Mean |
95% Confidence Interval of the Difference |
|||||
|
|
Lower |
Upper |
||||||
|
1day |
-2.20 |
1.58 |
0.28 |
-2.79 |
-1.60 |
7.60 |
29 |
0.000 S,p<0.05 |
|
1 month |
-31.50 |
3.09 |
0.56 |
-32.65 |
-30.34 |
55.77 |
29 |
0.000 S,p<0.05 |
|
2 month |
-34.36 |
3.89 |
0.71 |
-35.81 |
-32.91 |
48.38 |
29 |
0.000 S,p<0.05 |
|
3 month |
-55.50 |
8.40 |
1.53 |
-58.63 |
-52.36 |
36.17 |
29 |
0.000 S,p<0.05 |
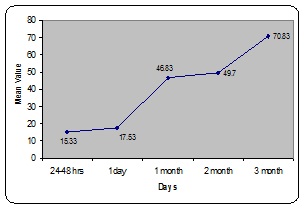
Graph 2: Comparison of Lysholm knee Scoring scale at 240-48 hrs, 1 day, 1 month, 2nd month and 3rd month
Mean Lysholm knee scoring scale at 24 – 48 hours was 15.33+-2.29 , at 1 day was 17.53 +-2.54, at 1 month was 49.70+- 3.45 and at 3 months was 70.83+-8.27. Significant difference is found at 1 day (t=7.60 , p =0.000) at 1 month (t=55.77 , p = 0.00), at 2 months (t=48.38 , p = 0.00) , and at 3 months (t= 36.17, p=0.00)
Table 3: Reliability Analysis of Lysholm knee scoring scale
Table 4 Comparison of Activity of daily living scale at 24-48 hrs, 1 day, 1 month, 2nd month and 3rd month
Descriptive Statistic
|
|
Mean |
N |
Std. Deviation |
Std. Error Mean |
|
24-48 hrs |
20.33 |
30 |
3.11 |
0.56 |
|
1day |
21.36 |
30 |
2.99 |
0.54 |
|
1 month |
48.73 |
30 |
2.53 |
0.46 |
|
2 month |
51.06 |
30 |
3.35 |
0.61 |
|
3 month |
72.86 |
30 |
7.70 |
1.40 |
Students paired t test
|
|
Paired Differences |
t |
df |
p-value |
||||
|
Mean |
Std. Deviation |
Std. Error Mean |
95% Confidence Interval of the Difference |
|||||
|
|
Lower |
Upper |
||||||
|
1day |
-1.03 |
0.49 |
0.08 |
-1.21 |
-0.85 |
11.54 |
29 |
0.000 S,p<0.05 |
|
1 month |
-28.40 |
4.12 |
0.75 |
-29.93 |
-26.86 |
37.70 |
29 |
0.000 S,p<0.05 |
|
2 month |
-30.73 |
5.24 |
0.95 |
-32.69 |
-28.77 |
32.09 |
29 |
0.000 S,p<0.05 |
|
3 month |
-52.53 |
6.65 |
1.21 |
-55.01 |
-50.04 |
43.21 |
29 |
0.000 S,p<0.05 |
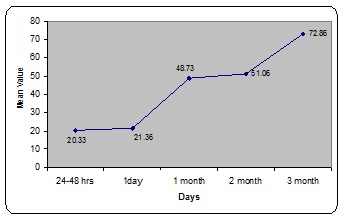
Graph 4: Comparison of Activity of daily living scale at 24-48 hrs, 1 day, 1 month, 2nd month and 3rd month.
Mean of Activity Of Daily Living Scale at 24 – 48 hours was 20.33+-3.11, at1 day 21.36+-2.99 , at 1 month 48.73+-2.53 , at 2 month 51.06+-3.35 and at 3month 72.86+- 7.70 . By using student paired t test significant difference was found at 1 day (t = 11.54, p = 0.00). At 1 month (t=37.70, p = 0.00), at 2month (t = 32.09 , p = 0.00) , at 3 month (t= 43.21 , p = 0.00)
Table 5: Reliability Analysis of Activity of daily living scale
Table 6: Correlation between Lysholm knee Scoring scale and Activity of daily living scale at 24-48 hrs, 1 day, 1 month, 2nd month and 3rd month
|
|
Lysholmknee Scoring scale
|
Activity of daily living scale |
Correlation |
p-value |
|
24-48 hrs |
15.33±2.29 |
20.33±3.11 |
0.12 |
0.51 NS,p>0.05 |
|
1 day |
17.53 ± 2.54 |
21.36 ± 2.99 |
0.04 |
0.81 NS,p>0.05 |
|
1 month |
46.83 ± 2.76 |
48.73 ± 2.53 |
0.90 |
0.00 S,p<0.05 |
|
2 month |
49.70 ± 3.45 |
51.06 ± 3.35 |
0.98 |
0.00 S,p<0.05 |
|
3 month |
70.83 ± 8.27 |
72.86 ± 7.70 |
0.94 |
0.00 S,p<0.05 |
Responsiveness was demonstrated by Spearman correlation for Lysholm Knee Scoring Scale and Activity of Daily Living Scale was ranging from (r =0.12 to 0.94) at 24 – 48 hours was 0.12 which is a weak correlation , on 1 day it was 0.04 which also states a weak correlation , 1 month it was 0.90 which means it had a strong correlation, 2 month it was 0.98 ,3 month 0.94 (which means at 2 month and 3month it had a strong correlation with each other )
DISCUSSION
The present study was undertaken in an attempt to find out the reliability and responsiveness of Lysholm knee scoring scale and Knee outcome survey activity of daily
living scale .In this study it is suggestive of that activity of daily living scale was superior to Lysholm knee scoring scale in assessing functional limitations in the wide
range of patient affected by anterior cruciate ligament injury26. Both the scales appears to be reliable, and responsiveness for the measurement of function related to
anterior cruciate ligament reconstruction. The main hypothesis in the study was supported (MAY ARNA et al 34)
The procedure used in this study was derived from the study done by JILL M MINKLEY et al (1999) activities of daily living scale is relevant instrument designed for
patients ranging from anterior cruciate ligament injury (ACL) to arthosis32.
Lysholm knee scoring scale is a 8 item questionnaire that was designed to evaluate patients after knee ligament surgery and it has been widely used for clinical research
studies27.
JAMES J IRRAGANG et al (1998) did a study on development of a patient reported measure of function of the knee, there main aim was to demonstrate responsiveness, reliability and validity of activities of daily living scale of the knee outcome survey, a patient reported measure of functional limitations imposed on patients with
pathological disorder and impairments of knee26. The scale was administered four times during an eight week period, at the time of initial evaluation and after one, four,
and eight week of therapy . They took additional 52 patients just to establish the test retest reliability and they finally made an conclusion that the scale was reliable, valid
and responsive for the assessment on the patients with disorder and impairments of the knee26.
In the present study the subjects were taken for assessment after anterior cruciate ligament reconstruction and was measured with the help of Lysholm knee scoring scale and activities of daily living scale. The scale was administered five times in a 3 month period , at the initial evaluation that is after 24 to 48 hours after reconstruction , one day , 1 month , 2 month , 3 month respectively .
In the present study the results were analysed upon the scores obtained from the assessment and correlation was taken out between the two scales and with an additional Prognostic Rating Scale to find out the sensitivity of the scale.
The present study demonstrated that both scales were reliable, responsive but there was a higher value for activity of daily living scale (0.97 to 0.99) as compared to the Lysholm Knee Scoring Scale (0.78 to 0.88)
Though both the scales were statistically significant but the Activity Of Daily Living Scale had a higher coefficient alpha (0.97 to 0.99) with higher standard error of measurement (1.11).The patient score was significantly better after 1months of treatment in Activities of Daily Living scale as compared after 1 months of Lysholm Knee Score
This suggest that the Activities Of Daily Living Score was better in assessing functional limitations in the wide range of patients affected by anterior cruciate ligament
reconstruction26. The Activity of Daily Living Scale did not demonstrate acceptable concurrent reliability and responsiveness in relationship with Prognostic Rating Scale. There was a weak correlation between the scores on Activity Daily of Living Scale and Prognostic Rating Scale.
In a previous study by HEVARD MOKSNES et al (2008) et al studied on individuals with anterior cruciate ligament deficient knee classified as noncopers may be candidates for nonsurgical rehabilitation and this was evaluated by using single legged hop test , the knee outcome survey activities of daily living scale , the global rating of knee function , and the number of episodes of giving way with this concluded that 70 % of the subjects were potential noncopers over true copers after one year following non operative treatment .But the patients with ACL reconstruction showed excellent knee function and were highly active at one year follow up and there
prognostic accuracy with the screening examination was also significant35.
At present there is lack of literature to estimate test retest reliability in patients who have a disorder that is truly stable over a longer period of time, such as those who have a chronic slowly progressive condition. Both the scales are useful in detaching problems in the patients suffering from disorders of knee but not in any other condition other than those affecting knee.
In future studies the additional testing should be done to demonstrate test retest reliability over a longer period of time and to determine the usefulness of the scale in the
other population26.
In our study ,we also used a rating of expected change as the theory for change .Spearman correlation coefficient between the rating of change and the physical function changes scores obtained at 3 months interval varied from (0.21 to 0.20) for Lysholm Knee Scoring Scale and (-0.02 to 0.20) for Activity Of Daily Living Scale. The present study results coupled with those of WESTAWAY et al, he also provided support for evaluating a measure's of sensitivity to change. The results of the studies suggest that a correlation coefficient of approximately 0.20 can be expected at the end of 3 months .This information is also useful for estimating sample size for future studies, where this scale is used for theory for change.
The above outcome of the present study are showing that activities of daily living scale has a greater capability in assessing the functional limitation in the wide range of patients affected by ACL injury . Though at end of the first day it was found that there was no significant difference of scores between the scales but with multiple repeated
assessment at 1st, 2nd month, 3rd month have shown that activities of daily living scale was more effective in assessing the functional limitations of the patient
To summarize that the Activities of Daily Living Scale is much more reliable, and responsive to changes in an individual’s level of function and the levels remain stable with the level of function is unchanged.
CONCLUSION
The present study was conducted to find out the reliability and responsiveness of Lysholm knee scoring scale and Activities of Daily Living Scale over the course of 3 months.
The results obtained from this study shows that the Activities of Daily Living Scale appear to be useful instrument for measurement of functional limitations during activities of daily living experienced by individuals who have undergone Anterior Cruciate Ligament Reconstruction.
The relation observed between Prognostic Rating Scale with Activity Of Daily Living Scale was found to be non significant which implies that the rating by these three different scale are not associated measure responses with period of time even though the reliability of Activity Of Daily Living Scale(0.98) was higher .
REFERENCES
1. Mak-Ham Lam, Daniel TP Fong. Knee stability assessment on anterior cruciate ligament injury: Clinical and biomechanical approaches. Sports Medicine, Arthroscopy, Rehabilitation, Therapy & Technology 2009;1:20.
2. Dekker R, Kingma J, Groothoff JW, Eisma WH, Ten Duis HJ. Measurement of severity of sports injuries: an epidemiological study. Clin Rehabil 2000;14:651-656.
3. Dekker R, Groothoff J, Sluis C, Eisma W, Ten Duis H. Long-term disabilities and handicaps following sports injuries: outcome after outpatient treatment. Disability Rehabilitation 2003;25:1153-1157.
4. Majewski M, Susanne H, Klaus S. Epidemiology of athletic knee injuries: A 10-year study. Knee Surg Sport Tr A 2006;13:184-188.
5. Veltri DM, Deng XH, Torzilli PA, Warren RF, Maynard MJ. The role of the cruciate and posterolateral ligaments in stability of the knee. A biomechanical study. Am J Sports Med 1995; 23:436-443.
6. Myklebust G, Bahr R. Return to play guidelines after anterior cruciate ligament surgery. Brit J Sport Med 2005;39:127-131.
7. Tour 2 India 4 health. Fore runner’s heath care consultants medi tours and heath tourism services. Available at www.tour2india4health.com
8. Markolf KL, Mensch JS. Stiffness and laxity of the knee- the contributions of the supporting structures. A quantitative in vitro study. J Bone Joint Surgery Am 1976;58:583
9. Anterior Cruciate Ligament Injury. Sports Medicine. Available at http://orthosurg.ucsf.edu/ patient-care/divisions/sports-medicine/conditions/ knee/anterior-cruciate-ligament-injury-acl/
10. Lygia Paccini Lustosa, Sérgio Teixeira da Fonseca. Reconstruction of the anterior cruciate ligament: impact of muscular and functional performances at the return to pre-injury activity level. Acta Ortop. Bras. 2007;15(5):280-284.
11. Puspinder S Bajaj. ACL injury, does it require surgery? Centre Of Arthroscopy, Sports Medicine & Joint Replacement.
12. Daniel, DM, Stone, ML, et al. Fate of the ACL injured patient. A Prospective outcome study. Am J Sports Medicine 1994; 22:632
13. Muneta T, Sekiya I et al. Two bundle reconstruction of the anterior cruciate ligament using semitendinous tendon with end buttons: operative technique and preliminary results. Arthoscopy 1999;15:618
14. Karim K and Peter B. Clinical sports medicine 3rd edition. Published by McGraw Hill, 2006, pp 1032. ISBN 007471520-8
15. Stretching, Flexibility & Sports Injury Management. ACL Injuries and Anterior Cruciate Ligament Rehabilitation. Available at http://www.sportsci.org/encyc/aclinj/aclinj.html http://orthopedics.about.com/cs/aclrepain/a/acl.htm
16. Peter J. Millett. Steadman Hawkins Clinic. ACL Reconstruction Rehabilitation Protocol. Orthop clin north Am 2002;33:675.
17. Jette AM. Physical disablement concepts for physical therapy research and practice. Phys Ther 1994; 74:380-386.
18. World Health Organization. International Classification. The sensitive of Impairments, Disabilities, and Handicaps. Geneva.
19. May A Risberg, lnger H et al. Prospective Study of Changes Impairments and disabilities After Anterior cruciate Ligament Reconstruction. Clin J Sports Med 1999;29(7):400-412
20. Christine M Bonci. Assessment and Evaluation of Predisposing Factors to Anterior Cruciate Ligament Injury. Journal of Athletic Training 1999;34(2):155-164.
21. Douglas R Keskula et al. Functional Outcome Measures for Knee Dysfunction Assessment. Journal of Atheletic Training 1996 June; 31(2):105-110.
22. Kelley G Fitzgerald, Scott M Lephart. Hop Tests as Predictors of Dynamic Knee Stability. Journal of Orthopaedic & Sports Physical Therapy 2001;31(10) :588-597
23. Barker KL, Lamb SE et al. Repeatability of goniometer measurements of the knee in patients wearing an Ilizarov external fixator: A clinic-based study. Clin Rehabil 1999 Apr;13(2):156-63.
24. Michael A, Watklns Dan L Riddle. Reliability of goniometric measurements and visual estimates of knee range of motion obtained in clinical settings. Phys Ther. 1991;71:90-97.1.
25. Cross MJ, Wootton JR, Bokor DJ, Sorrenti SJ. Acute repair of injury to the anterior cruciate ligament. A long-term followup. Am J Sports Med. 1993 Jan-Feb;21(1):128-31.
26. James J, Irrgang, Pittsburgh, lynn S. Development of a patient reported measure of function of the knee. The journal of bone and joint surgery. 1998;80 :1132-45
27. Robert G Marx. Knee rating scale .Isakos Scientfic Committe Report. The Journal of arthroscopic and related surgery December 2003; 19(10): 1103–1108.
28. Bellamy N, Buchanan WW, Goldsmith CH, Campbell J, Stitt LW. Validation study of WOMAC: a health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee. J Rheumatol Dec 1988;15(12):1833-40.
29. Noyes FR, McGinniss GH, Mooar LA. Functional disability in the anterior cruciate insufficient knee syndrome. Review of knee rating systems and projected risk factors in determining treatment. Sports Med. Jul-Aug 1984;1(4):278-302.
30. Tegner Y, Lysholm J. Rating systems in the evaluation of knee ligament injuries. Clin Orthop Relat Res. Sep 1985;(198):43-9.
31. Andrea R, Trevor B Birmingham. Hop testing provides a reliable and valid outcome measure during rehabilitation after anterior cruciate ligament reconstruction. Physical therapy journal March 2007; 87:337-349.
32. Jill M Binkley, Paul W Stratford. The lower extremity functional scale (LEFS): scale, development, measurement properties, and clinical application. Phys therapy journal April 1999;79(4): 371-383.
33. Westaway M, Stratford PW. The patient specific functional scale : validation of its use in persons with neck dysfunction. Journal of orthopaedics and sports physical therapy 1998;27:331-338.
34. May A Risberg , Inger H. Neuromuscular training versus strength training during first 6 months after anterior cruciate ligament reconstruction: a randomized clinical trial. Physical therapy 2007 June; 87(6):738-750.
35. Havard M, Lynn S Mackler. Individuals with an anterior cruciate ligament deficient knee classified as non copers may be candidates for non surgical rehabilitation. Journal of orthopaedics and sports physical therapy 2008 Oct; 38(10): 586–595.